
Non-Surgical Treatments for Herniated Discs
Herniated intervertebral discs are a common cause of back pain and disability, impacting a vast number of people globally [1]. These discs, acting as cushions between vertebrae, are essential for spinal movement and shock absorption [2]. Understanding the structure of these discs is key to understanding the mechanisms behind disc herniation.
Disc Structure and Degeneration
The intervertebral disc consists of two main parts: the annulus fibrosus, a tough outer layer, and the nucleus pulposus, a gel-like core [3]. The nucleus pulposus is primarily composed of type II collagen and proteoglycans and contains a high percentage of water [4]. This composition allows the disc to absorb shock and distribute loads effectively. The annulus fibrosus is made up of layers of collagen fibers that encase and contain the nucleus pulposus [2, 3].
Over time, a process called disc degeneration can occur, characterized by biochemical and biomechanical changes in the disc [5]. The nucleus pulposus loses water content and proteoglycans, becoming less resilient and compromising its shock-absorbing capacity [5, 6]. The collagen fibers in the annulus fibrosus can degrade, leading to weakness and tears in the outer layer [7].
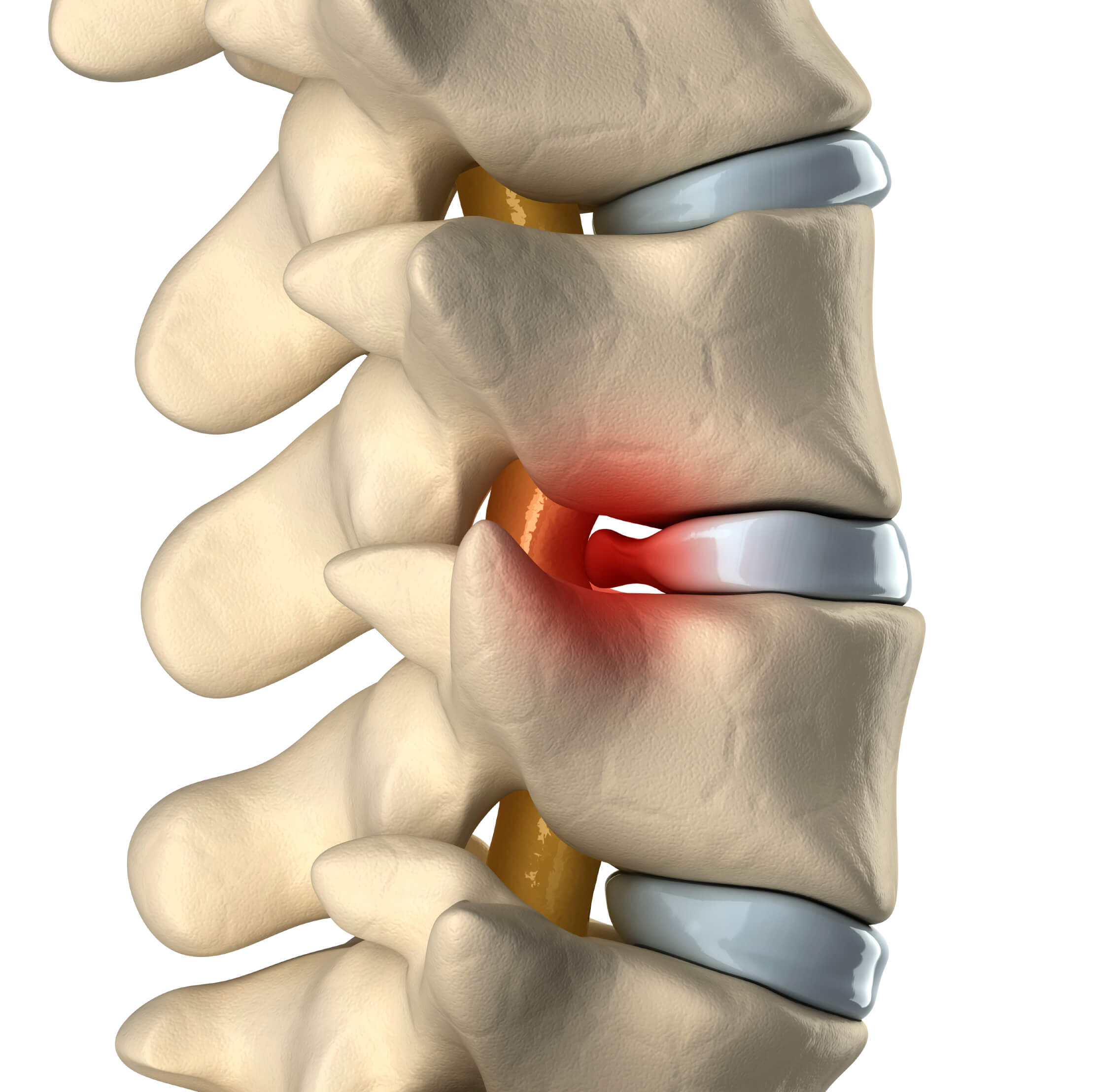
The Mechanics of Herniation
When the annulus fibrosus weakens, the nucleus pulposus can protrude through these tears or weak spots, leading to a herniated disc [2, 3]. This protrusion can compress nearby nerve roots, causing pain, numbness, tingling, and even muscle weakness [2]. The location of the herniation determines the specific symptoms experienced [2]. For example, a lumbar disc herniation can result in sciatica, characterized by pain radiating down the leg [2, 8]. A cervical disc herniation can cause pain and neurological symptoms in the neck, shoulder, and arm [2]. If left untreated, prolonged nerve compression can lead to permanent damage [8].
Risk Factors
Several factors can contribute to disc degeneration and herniation. These include:
- Aging: The natural aging process leads to changes in disc composition and structure, making discs more susceptible to degeneration [5].
- Genetics: Some individuals may have a genetic predisposition to disc problems [9].
- Lifestyle factors: Occupations involving prolonged sitting, repetitive heavy lifting, or other physically demanding tasks can significantly increase the risk of disc herniation [10]. Smoking and obesity are also associated with an increased risk [9].
- Trauma: A sudden injury or impact to the spine can cause a disc to herniate [9].
Non-Surgical Treatment Options
While surgery is sometimes necessary for severe cases, non-surgical treatments are often the first line of management for herniated discs [11]. These treatments can range from conservative management to minimally invasive procedures [11, 12].
1. Conservative Management: This approach focuses on pain relief, reducing inflammation, and promoting healing without invasive procedures. It typically involves:
- Rest: Short periods of rest can help alleviate acute pain, but prolonged bed rest is not recommended [9].
- Medications: Over-the-counter pain relievers like nonsteroidal anti-inflammatory drugs (NSAIDs), muscle relaxants, and neuropathic pain medications can help manage pain [9].
- Physical Therapy: A structured physical therapy program is crucial for strengthening core muscles, improving flexibility, and promoting proper posture, which can help stabilize the spine and reduce stress on the discs [9].
- Activity Modification: Avoiding activities that worsen pain is important to allow the disc to heal [9].
Conservative management is generally recommended for patients with mild to moderate pain, contained herniations, and no significant neurological deficits [13]. If symptoms persist despite 4-6 weeks of conservative treatment, other interventions may be considered [13].
2. Minimally Invasive Procedures: When conservative management is not sufficient, minimally invasive procedures offer a less invasive alternative to open surgery. These procedures typically involve inserting small instruments into the disc under image guidance. The choice of procedure depends on the type and severity of the herniation and the patient’s symptoms [14].
Key Minimally Invasive Techniques
- Disc Aspiration: This procedure involves removing a portion of the nucleus pulposus using a small needle to reduce disc volume and relieve pressure on the nerves [15]. It is a quick outpatient procedure with minimal recovery time [15].
- Disc Vaporization (Nucleoplasty): This technique uses radiofrequency energy to ablate and vaporize a portion of the nucleus pulposus, reducing pressure within the disc and relieving nerve compression [16]. It is performed under local anesthesia, and patients usually go home the same day [16].
Other Minimally Invasive Options:
- Chemonucleolysis: This technique involves injecting an enzyme into the disc to break down the nucleus pulposus, reducing disc volume and pressure. However, it carries a risk of allergic reactions and is less commonly used now [17].
- Percutaneous Laser Disc Decompression (PLDD): This procedure uses laser energy to vaporize a small portion of the nucleus pulposus. It is generally safe and effective for contained herniations [18].
- Intradiscal Electrothermal Therapy (IDET): This technique uses heat to modify the collagen fibers within the annulus fibrosus, potentially shrinking the disc and reducing pressure [19].
- Epidural Steroid Injections: While not directly targeting the disc, these injections deliver corticosteroids to the area surrounding the nerve roots, reducing inflammation and providing temporary pain relief [20].
Choosing the Right Treatment:
Selecting the most appropriate treatment depends on factors such as the type and severity of the herniation, the patient’s symptoms, overall health, and response to prior treatments [14]. A stepped approach is often recommended, starting with conservative management and progressing to minimally invasive procedures if necessary [9].
Success Rates and Potential Risks:
Minimally invasive procedures have shown promising results in relieving pain and improving functionality [21]. They generally have lower risks of complications and shorter recovery times compared to traditional open surgery [21].
- Disc vaporization, for example, has demonstrated an 80% success rate in symptom relief, compared to a 65% success rate with traditional surgeries [22]. Patients typically return to normal activities within 10 days [22].
- In a clinical study, disc vaporization resulted in a quicker return to work (average 10 days) compared to open surgery (average 4-6 weeks), with similar success rates in pain relief but a significantly lower risk of complications [16].
However, it’s important to note that all procedures carry potential risks and complications, although these are generally less frequent and severe than those associated with open surgery [23].
Potential Risks of Minimally Invasive Procedures:
- Disc Aspiration: Potential complications include discitis (infection), bleeding, nerve root injury, and recurrent herniation [23, 24]. The reported incidence of discitis is between 0.1-2%, while nerve injury is rare at less than 1% [24]. Recurrence of herniated disc symptoms after disc aspiration is reported in about 5-15% of cases [24].
- Disc Vaporization: Risks include discitis, nerve injury due to thermal damage, and recurrent herniation. The incidence of these complications is generally low, with nerve injury occurring in less than 1% of cases [21, 25]. Recurrence rates are similar to those of disc aspiration [24].
- Chemonucleolysis: The primary risk is allergic reaction, including the rare but serious complication of anaphylaxis [25]. Discitis and nerve root injury can also occur [25].
- PLDD and IDET: These procedures carry similar risks to nucleoplasty, including discitis, nerve injury, and recurrent herniation [26]. The incidence of these complications is generally low [26].
- Epidural Steroid Injections: Risks include infection, bleeding, nerve injury, dural puncture headache, and a temporary increase in pain [26]. The incidence of serious complications is generally low [26].
Surgical Intervention:
Surgery is usually considered when:
- Cauda Equina Syndrome: This condition involves compression of the cauda equina nerves at the base of the spinal cord, leading to bowel or bladder dysfunction, saddle anesthesia, and lower extremity weakness [14]. It requires emergency surgery [14].
- Progressive Neurological Deficits: Worsening weakness, numbness, or changes in reflexes require prompt surgical evaluation [14].
- Intractable Pain: When severe pain doesn’t respond to conservative and minimally invasive treatments, surgery may be warranted [14].
- Large Herniations or Instability: Certain large herniations or spinal instability may require surgery for optimal management [14].
Future Directions:
The field of non-surgical treatments for herniated discs continues to evolve with advances in technology and research.
- Technological Advancements: Innovations like low-bit energy radiofrequency ablation and robotic-assisted guidance systems may enhance precision and safety in minimally invasive procedures [26].
- Regenerative Therapies: The combination of minimally invasive procedures with regenerative therapies, such as stem cell injections, holds potential for long-term disc repair [7, 26]. Early trials using mesenchymal stem cells have shown promising results in pain relief and disc height improvement [27]. Other biological therapies under investigation include platelet-rich plasma (PRP) and bone morphogenetic proteins (BMPs) [27]. Gene therapy and novel drug delivery systems are also being explored [27].
- Clinical Trials and Long-Term Data: While early clinical trials on stem cell injections have shown encouraging results, with reports of 70% improvement in pain scores at 12 months post-injection, more research is needed to determine the long-term efficacy and safety of these regenerative therapies [28].
The Importance of Continued Research:
Despite the promising short-term results of many non-surgical treatments, further research on long-term outcomes is crucial. Areas of focus include:
- Recurrence Rates: Understanding the long-term recurrence rates of herniated discs after different treatments is essential for informing patient expectations and treatment decisions [29].
- Functional Recovery: Assessing the long-term impact of these treatments on patients’ functional abilities and quality of life is critical [29].
- Patient Satisfaction: Gathering data on patient satisfaction with different treatment modalities can help guide treatment recommendations and improve patient care [29].
- Standardization: As non-surgical techniques become more widespread, developing standardized treatment protocols is becoming increasingly important to ensure consistent outcomes and facilitate comparisons across different therapies [29].
Conclusion:
Non-surgical treatments for herniated discs have significantly advanced, offering effective alternatives to traditional surgery. These treatments provide pain relief, improved function, and reduced recovery times. Continued research into long-term outcomes, regenerative therapies, and standardized protocols will further refine these approaches, ensuring that patients receive the most effective and safest care possible.